45 year old male with abdominal distension
DR.NAVYA(INTERN)
DR.CHETANA(INTERN)
DR.ABDUL RAHEEM (INTERN)
DR.ASHFAQ(INTERN)
DR.SRAVYA(INTERN)
DR.GNANADA(INTERN)
DR.CHARAN(PG1)
DR.VAMSI(PG1)
DR.SUSMITHA(PG2)
DR.ADITHYA (PG3)
DR.PRANEETH(PG3)
DR.PRAVEEN NAIK (ASS.PROF)
DR.RAKESH BISWAS(HOD)
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
Unit 1 admission on 22/2/21
A 45 yr old male patient came with chief c/o yellowish discolouration of sclera since 20 days
Abdominal distension since 20 days
Pedal edema since 20 days
SOB since 15 days
HOPI-
Pt was apparently asymptomatic 5 years back then he developed vomitings , went to hospital, where he was told low bp, hypokalemia, liver disease. Then he recently developed similar complaints associated with jaundice
20 days back he developed abdominal distension,yellowish discolouration of sclera and urine associated with b/l pitting type of pedal edema up to knee
No history of chest pain ,hemoptysis, abdominal pain , burning micturition ,increased frequency of micturition or urgency
Past history -
Not a k/c/o HTN,DM,BA,TB
Personal history-
Diet -mixed
Appetite- normal
Bowel and bladder movements-regular
Consumption of 360ml of whiskey per day since 15 years
Chewing of gutka since 10 years
No known allergies
General examination
Pt is conscious, coherent, cooperative
Weight -53 kgs , height -165cms
BMI-19.4
B/l pitting type of edema up to knee - present
Icterus +
No signs of pallor, cyanosis, generalised lymphadenopathy
Vitals -
Bp-110/70mmhg
PR-92 bpm
RR-18cpm
Temp - afebrile
Spo2-91% at RA
GRBS-138 mg/dl
General Examination:
Icterus present
Temporal wasting present
Loss of buccal pad of fat and axillary fat
B/L parotid enlargement
Gynecomastia
Palmar erythema present
Respiratory-
Dyspnea- present
Centrally positioned trachea
Vesicular breath sounds
are heard
No added sounds
P/A- inspection
Shape of abdomen- distended , with abdominal girth of 85cm
Umbilicus-slit like
Non tender , visible distended veins , multiple scars over abdomen are present , no visible sinuses
Palpation -
Mild hepato and splenomegaly
Percussion - shifting dullness present
Auscultation- bowel sounds +
CVS-S1,S2 +, no murmurs
CNS- NAD
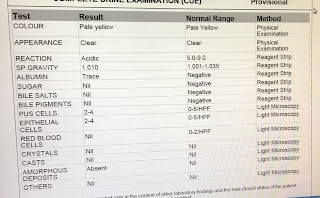
Investigations:















provisional diagnosis-
CIRRHOSIS WITH PORTAL HYPERTENSION secondary to ALCOHOL

Comments
Post a Comment